
Dating as a resident physician is not the scheduling problem most residents assume it is. 72.8% of resident physicians are already partnered or cohabitating. In PGY-1 alone, 27.7% of residents get married, nearly double the 13.9% who break up. Intern year does not destroy relationships. It stress-tests them. The ones built on a real foundation survive. The ones without a foundation dissolve.
My name is JT Tran. I am a dating coach who has spent nearly two decades working with high-achieving men, doctors, engineers, lawyers, and executives who are exceptional at everything their profession demands and chronically underdeveloped in the one area their training never addressed. At 5’4″ and not conventionally attractive by any standard, I have been the shortest man in the room, the least noticed, and the one nobody expected to be talking to women at all. The system I built exists specifically because the gap between achievement and attraction is not a personality defect. It is a skills gap. And unlike your Step 1 score, this one is actually fixable.
Two Doctors. Two Outcomes. One Difference.
Two of my clients are doctors who went through residency in completely different ways. Jimmy built his dating life during medical school. He took the ABCs of Attraction bootcamp, then the EuroTour. By the time residency started he had a foundation in place. The hours did not disappear. The pressure did not disappear. But the social skills and the confidence he had built compounded through the clinical years rather than stalling out in them. He started building during pre-med and carried that foundation through medical school. The full story is in our dating as a medical student article.
Jared took the other path. He deferred through medical school, told himself there was no time, arrived at residency without a foundation, and deferred again. He came to us after a seven-year rut with no girlfriend and no real framework for building one. Three days at our Miami bootcamp transformed his body language and his willingness to approach women he would never have approached before. He described it as life-changing. But the deficit he accumulated by waiting is real and it compounds. Every year he deferred is a year of skills he did not build and reps he did not accumulate.
The difference between Jimmy and Jared is not intelligence. Not talent. Not the specialty they matched into. It is what they built and when they built it.
This article covers what dating during residency actually looks like by the numbers, why the hours are not the variable most residents think they are, what intern year specifically does to relationships, where residents actually meet people, and how the ABCDEF System addresses the specific patterns residency training creates.
Read it as a second opinion on the belief that has been keeping you stuck. The data on dating as a resident physician is more specific and more actionable than most residents expect.
What Dating as a Resident Physician Actually Looks Like by the Numbers
The data on dating during residency tells a more complicated story than most residents expect. 92.4% of medical students enter training single. Yet by PGY-5, 61.6% of residents are married. That is not a coincidence. Residency is not the dead zone for relationships that most residents assume it is. It is the primary window in which most physicians form their long-term partnerships.
The men who are succeeding at dating as a resident physician are not outliers. By the time training ends, they are the majority. Whether it is possible is not the question. The real question is whether you are on that trajectory right now and if not, why not.
The Hours Are Not the Variable
The 72.8% of residents who are currently partnered or cohabitating are not in easier programs. They are not in less demanding specialties. The data from peer-reviewed research shows that the weekly work hours between specialties with dramatically different quality of life outcomes differ by less than one minute. 78.33 hours versus 78.35 hours. The hours are virtually identical. The outcomes are not. Which means the hours are not the variable driving relationship outcomes during residency. Something else is.
That something else is what this article is about.
Dating During Residency: What the First Year Actually Does
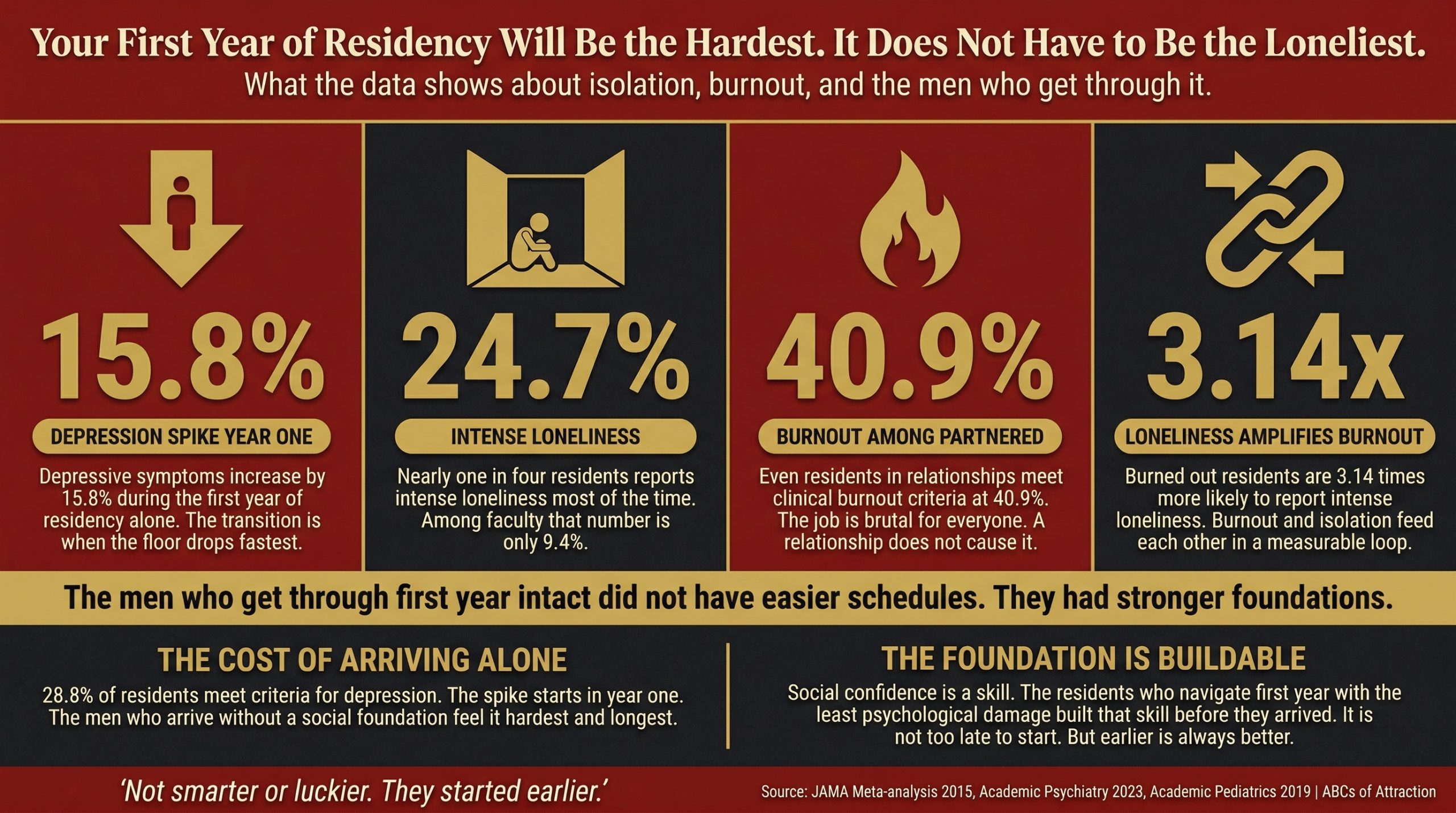
Source: Archives of Internal Medicine 2010, Academic Psychiatry 2023, Academic Pediatrics 2019. Depression spikes 15.8% in the first year alone. The men who get through it intact did not have easier schedules. They had stronger foundations.
The transition from MS4 to PGY-1 is the most socially disruptive event in the entire medical training pipeline. On Match Day your cohort from medical school scatters across the country. You arrive in a new program, often a new city, with co-residents you did not choose and an attending hierarchy you are at the bottom of. The social world you spent four years building disappears in a single day.
What happens next is documented. 35% of interns screen positive for clinically significant depression within their first year. Depressive symptoms increase by a median of 15.8% during that transition alone. Furthermore, 24.7% of residents report intense loneliness a lot or most of the time, compared to only 9.4% of faculty. The gap between where you are and where your attendings are psychologically is not just experience. It is the measurable cost of arriving without a social foundation in an environment that provides almost no scaffolding for building one.
The research from Academic Medicine identifies what they call a hierarchy of relationships during residency. Professional identity systematically supersedes personal relationships not because residents stop caring about connection but because the training environment rewards clinical performance and provides no framework for social development. You are trained to be a physician. Nobody trains you to maintain a relationship under these conditions or build one from scratch in a new city with people you met three weeks ago. Your program director has a lot of opinions about your case presentations. Zero opinions about your dating life. On that front, you are entirely on your own.
The men who navigate intern year with the least psychological damage are not the ones in the easiest programs. They are the ones who arrived with something already built.
The PGY-1 Stress Test: Why Intern Year Reveals Everything
Here is the data point most residents never see. In PGY-1, 27.7% of residents get married. In that same year, 13.9% break up. Intern year is not when relationships end. It is when they get sorted. The relationships with a real foundation survive the pressure and often accelerate toward commitment. Those built on proximity and convenience without a genuine foundation dissolve under the same pressure.
Therefore, the implication for men who are single going into residency is direct. The stress of intern year does not make building a relationship harder in some abstract future sense. It makes it harder right now, in the year when the psychological floor drops fastest and the social world is smallest. The men who arrive without a foundation are navigating the hardest year of their training with the lowest social resources at exactly the moment when those resources matter most.
And the cost compounds. If you are depressed as an intern and do not have a relationship functioning as a psychological buffer, research from the Intern Health Study shows your depression scores remain three times higher five years later. This is not a transient rough patch that residency produces and time heals. It is a psychological trajectory that sets the tone for the entire training period and beyond.
Jared arrived at residency having deferred through all four years of medical school. Intern year hit him exactly the way the data predicts. The hours were brutal, the social world was new and unfamiliar, and he had no foundation to fall back on.
He told himself it would get better after intern year. It did not get better. The deficit compounded. He repeated that logic through residency, then through fellowship, until he finally showed up at our Miami bootcamp after seven years wondering why the schedule never seemed to clear enough to start.
The Hours Myth: Why Dating in Residency Is Not a Scheduling Problem
56.1% of single medical students cite career focus, as documented in our dating as a medical student research, as the primary reason they are not dating. Most carry that belief directly into residency and add the hours as additional justification. Nobody is arguing otherwise. The schedule is brutal, the exhaustion is real, and the emotional bandwidth after a 28-hour call is genuinely low. If you have ever tried to be charming at 6am after a night shift, you already know exactly what low emotional bandwidth feels like.
But consider what the data actually shows about hours and outcomes. The weekly work hours between residency specialties with dramatically different quality of life scores differ by 0.02 hours. Less than two minutes per week. Two minutes. The specialties where residents report the lowest quality of life are not the ones working the most hours. They are the ones with the least autonomy and the highest intensity.
The variable driving quality of life during residency is not total hours. It is the experience of those hours. Understanding that distinction is the foundation of everything that works about dating as a resident physician.
The Time You Actually Have
The residents who are in relationships are not working fewer hours than the ones who are single. They have 17 to 25 hours of discretionary time per week after work, sleep, and basic hygiene, the same as everyone else in their program. The question is what that time is being spent on.
There is a finding in the research that most residents never encounter. Single residents are significantly less likely to look forward to going to work than partnered residents, despite having less family strain on their schedule. In other words, being single does not make the workload easier to bear. It makes the experience of residency measurably worse. The relationship is not competing with residency for your limited resources. It is what makes those resources go further.
17 to 25 hours per week is more than most residents assume they have. The men who are building relationships during residency are not finding secret pockets of time that do not exist for everyone else. They are making a specific allocation decision with the same discretionary hours every resident has. Two hours of that redirected from consumption to genuine social investment changes the entire equation.
The Relationship as Protection: What the Data Shows About Dating as a Resident Physician
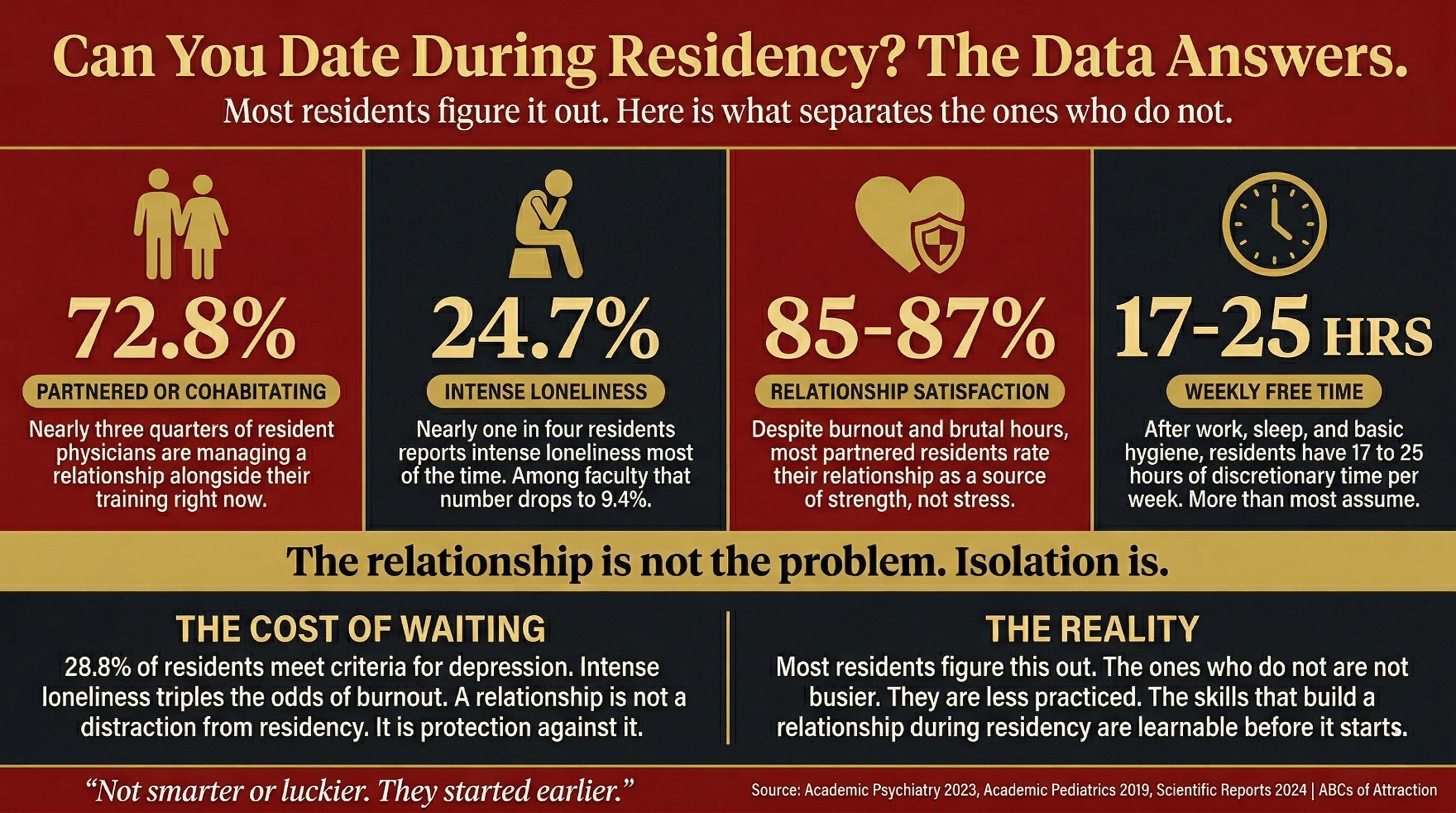
Source: Academic Psychiatry 2023, Academic Pediatrics 2019, Scientific Reports 2024. Nearly three quarters of resident physicians are in a relationship right now. The ones who are not are not busier. They are less practiced.
40.9% of partnered residents meet clinical criteria for burnout. The relationship is not protecting them from burnout. The job produces burnout regardless of relationship status. What the relationship does is change how burnout is experienced and how long its effects persist.
Think about what that actually means. You can be burned out and deeply satisfied in your relationship at the same time. Most residents assume these two things cannot coexist. The data says otherwise.
85% to 87% of partnered residents report high relationship satisfaction despite the pressure of training. The relationship is the sanctuary, not the burden. And the effect extends beyond personal life into professional performance. Married residents report being happy at work at a rate of 76.8% compared to 70.2% for single residents. Program fit follows the same pattern: 88.5% of married residents feel they belong in their program compared to 81.6% of single residents. The relationship does not just make the personal hours better. It makes the clinical hours better.
Burned out residents are 3.14 times more likely to report intense loneliness than residents who are not burned out. Burnout and isolation feed each other in a measurable loop. As a result, the men who arrive at residency without a social foundation and without the skills to build one do not just have a harder personal life. They have a harder residency.
When the Hours Are Brutal and the Relationship Survives Anyway
The research even documents this in extreme conditions. Among neurosurgery residents working 80-plus hour weeks, 84% of their partners report high relationship satisfaction. The hours are not destroying these relationships. Instead, the quality of what was built before and during those hours is what matters.
A relationship is not a luxury you earn after residency gets easier. It is protection against the most psychologically demanding period of your career. The men who treat it as a reward for surviving residency are making the survival harder than it needs to be.
Where Resident Physicians Actually Meet People to Date
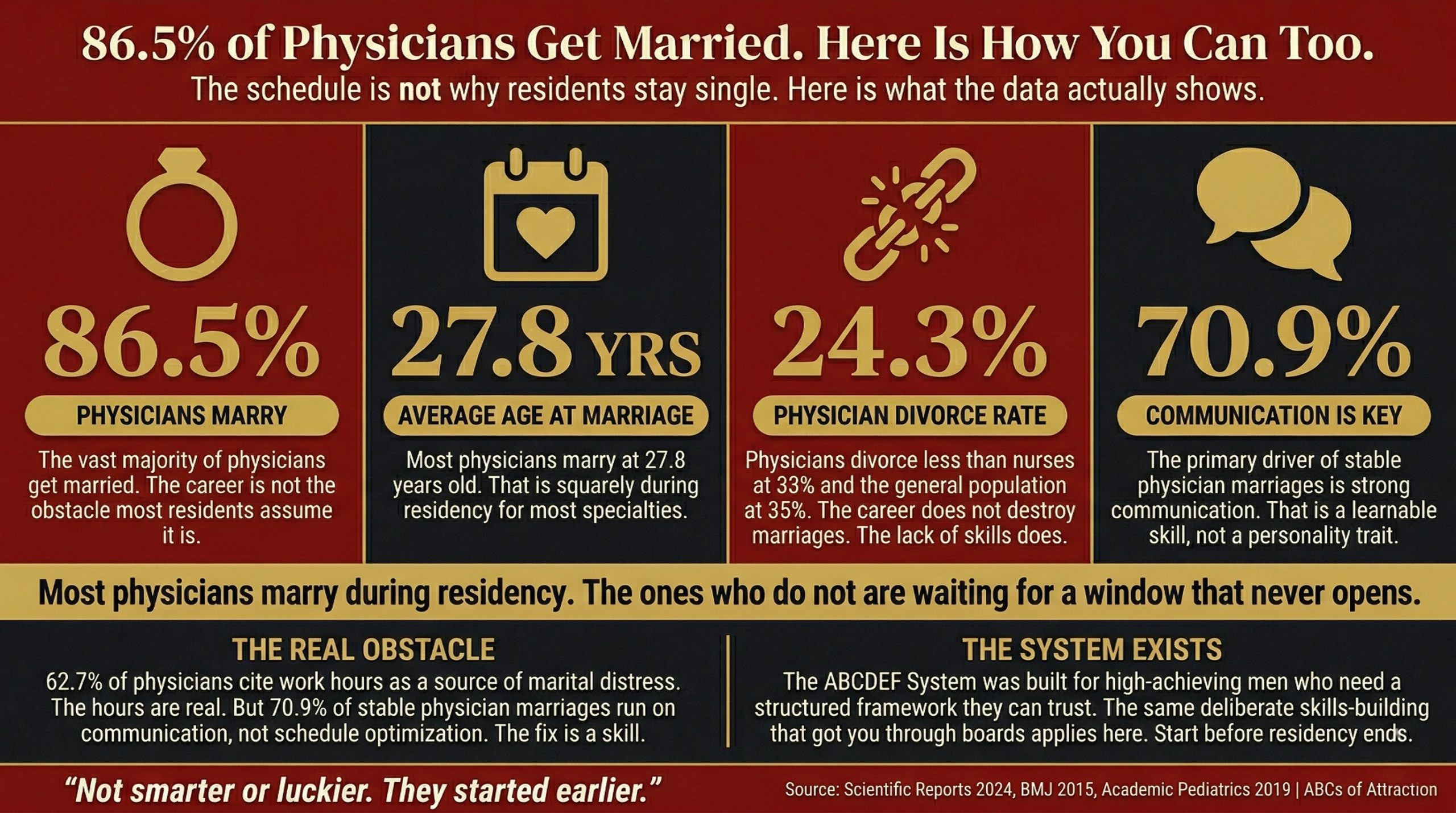
Source: Scientific Reports 2024, BMJ 2015, Academic Pediatrics 2019. Most physicians marry during residency. The ones who do not are waiting for a window that never opens.
The same research that documents loneliness and burnout during residency also shows that 41.7% of PGY-1 residents are already married, rising linearly to 61.6% by PGY-5. These men are meeting people somewhere. The question is where. Spoiler: it is not primarily Hinge.
The hospital during residency is the richest social environment most resident physicians will ever consistently inhabit. You are no longer a medical student rotating through for a few weeks. You are a physician with authority, a white coat that carries real professional status, and recurring relationships with nurses, attendings, fellows, and co-residents that build over months rather than weeks.
The attending who watched you handle a difficult patient on an overnight shift is not just a supervisor. She is someone who has seen you perform under pressure and carry yourself with composure. That is the most credible social proof available and it exists nowhere outside the hospital. The social conditions inside, shared mission, high emotional stakes, mixed gender, recurring proximity, are almost perfectly designed for fast genuine connection.
The 81.2% of partnered medical students who met through friends and the 80.2% who met through social outings carry directly into residency. Consequently, your program social events, your co-resident relationships, the small margins between shifts, the shared experience of a brutal overnight or a difficult patient are not incidental social opportunities. They are the primary social environment of your life during training and the men who treat them as purely professional are opting out of the only consistent social world they have access to.
Dating apps remain a supplement, not a strategy. A physician-specific dating app called DownToDate has over 5,000 verified physician users, which tells you the demand exists. Apps are a useful gap-filler between real social interactions. However, the men who rely on them as a primary channel during residency are making the same mistake our medical student research documents: 66.3% use apps but 81.2% met their partner through friends. Those are not the same men.
The Match Complication
Beyond the day-to-day social environment, the Match adds a specific complication. Long distance is the number one cause of relationship breakdown during medical training at 36.9%, with futures diverging at 34.4% close behind. Both are Match-related pressures. The men who arrive at fourth year with a relationship built on a real foundation and real skills navigate the Match from a position of strength. The men who arrive having deferred face those pressures without the stabilizing effect of anything they have built.
Why Dating as a Resident Physician Feels Impossible: The Real Reason
The men who struggle most with dating in residency are not struggling because their schedule is too demanding. The data has already established that the hours are virtually identical between residents with dramatically different relationship outcomes. They are struggling because the skills that made them exceptional physicians are almost perfectly designed to fail them in dating.
This is not an insult. It is a mechanical observation. The same training that makes you good at one thing makes you bad at another. A surgeon who has spent five years developing steady hands and zero emotional reactivity in the OR is not a worse human being for those years. He is just carrying habits into a context where they actively work against him.
Medicine rewards precision, hierarchy, deference, and emotional suppression. Three to seven years of residency training does not just teach clinical skills. As a consequence, it trains specific behavioral patterns that become deeply entrenched. You learn to suppress uncertainty, to operate within hierarchy, to present competence rather than vulnerability. Emotional exposure becomes a liability in the clinical environment, and that lesson does not stay in the hospital.
In short, dating requires the exact opposite of all of those patterns. Presence over precision. Spontaneity over deference. Vulnerability over competence performance. The willingness to tolerate uncertainty without spiraling into clinical assessment mode.
Where Resident Physicians Stall in the ABCDEF System
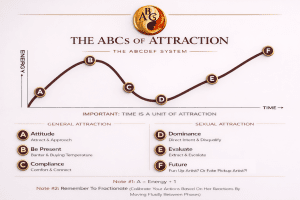
The ABCDEF System addresses this mismatch phase by phase. It is not a script. It is a diagnostic tool that tells you exactly which skill is missing and gives you a concrete drill to develop it in the specific conditions of your life right now.
The A phase, Attitude, Attract, Approach, addresses the internal state before any interaction. For most residents the internal state before approaching a woman after a 28-hour call is not attraction. It is survival mode. Switching psychological gears between clinical and social environments is a specific learnable skill that most residents have never been taught because nobody in their training chain does it either.
The B phase, Be Present, Banter, Buying Temperature, is where residents collapse most consistently. You are not trying to impress her with your board scores or your research output. Instead, you are trying to make her laugh about something that happened on rounds this morning. Presence and playfulness under conditions of genuine exhaustion is a skill. It is learnable. It is almost the exact opposite of what three to seven years of residency training has been building in you.
The C phase, Compliance, Comfort, Connect, and the D phase, Dominance, Direct Intent, Disqualify, address the two patterns residency creates most reliably. Years of operating within hierarchy produce men who listen exceptionally well and escalate never. Years of clinical deference produce men who are warm, attentive, and completely unreadable as romantic interests. These are the two phases where resident physicians stall hardest and where the right coaching produces the fastest results.
Here is the short version: you have spent years learning to be the most competent, least threatening person in every room. That is exactly what a good resident does. Unfortunately, it is also exactly what keeps you in the friend zone. The D phase teaches you how to stop being the world’s most qualified emotional support animal and start being someone a woman is actually attracted to.
For a deeper breakdown of where the internal patterns driving this behavior actually come from, read this article on the inner game collapse and what actually drives the behavior you are trying to change.
Five Things to Do This Week to Improve Dating as a Resident Physician
The data tells you why. Here is what to do with it this week, not after the next rotation, not after boards, this week.
1. Map Your Time: The First Step to Dating During Residency
Not estimated. Actual. Track every hour outside of clinical work and sleep for seven days. Most residents who run this audit find 17 to 25 hours of discretionary time they did not know they had. Two hours of that redirected from screens to genuine social investment changes the entire equation. You cannot solve a problem you have not accurately diagnosed.
2. Identify one environment in your program you are treating as purely professional
The hospital, your co-resident group, your program social events. Pick one environment where you currently operate in clinical mode exclusively and make one genuine non-clinical connection this week. Not a big approach. One real conversation that has nothing to do with medicine. The men who are building relationships during residency are using the same environments you are already in. They are just being present in them differently.
3. Practice switching gears between clinical and social mode deliberately
The transition from 28-hour call to a social environment is a specific psychological shift that most residents never practice. This week, identify one moment after a clinical shift where you deliberately switch modes before engaging socially. The B phase of the ABCDEF System is built around this transition. Presence under exhaustion is a learnable skill. The first step is noticing when you are still in clinical mode in a social environment.
4. Run the numbers on what waiting is actually costing you
Marriage rates among residents increase linearly from 41.7% in PGY-1 to 61.6% in PGY-5. If you are in PGY-2 or beyond and not on that trajectory, every rotation you defer is a rotation of compounding deficit. If you are depressed as an intern without a relationship as a buffer, research shows your depression scores remain three times higher five years later. The cost of waiting is not abstract. It is measurable, documented, and it compounds. Run the actual math on where you will be at the end of fellowship if the current trajectory continues unchanged.
5. Start Now: Dating as a Resident Physician Does Not Get Easier Later
The window you have right now is not the easiest window you will ever have. That window was medical school, and if you are still there, our dating as a medical student article is where to start. If you started before med school even began, our pre-med dating advice covers the earliest and most leveraged window of all.
But the window you have right now in residency is still easier than fellowship, and significantly easier than attending life. The men who arrive at each new phase of training having built something navigate it differently than the men who arrive having deferred again. The next rotation starts soon. Apply for a free coaching call before it does, not after.
Frequently Asked Questions: Dating as a Resident Physician
Can you date during residency?
Yes. 72.8% of resident physicians are currently partnered or cohabitating. By PGY-5, 61.6% of residents are married. Dating during residency is not the exception. It is what the majority of residents figure out over the course of their training.
Do residents have time to date?
After work, sleep, and basic hygiene, residents have 17 to 25 hours of discretionary time per week. The men who are in relationships during residency are not finding time that does not exist for everyone else. They are making a specific allocation decision with the same hours every resident has.
Does residency ruin relationships?
The data does not support this. 85% to 87% of partnered residents report high relationship satisfaction despite the pressure of training. 84% of partners of neurosurgery residents, who work 80-plus hour weeks, report high satisfaction. Residency stress-tests relationships. It does not systematically destroy them.
When is the best time to start dating during residency?
Before residency starts. The men who arrive at PGY-1 with a social foundation already in place navigate intern year differently. For men already in residency, the best time is now rather than after the next rotation. Marriage rates increase linearly through training. The men on that trajectory started building at some point. That point can be now.
What specialties have the best work-life balance for dating?
The research shows that weekly work hours between specialties with dramatically different quality of life outcomes differ by less than two minutes per week. The variable driving relationship outcomes during residency is not the specialty chosen. It is the skills and foundation brought into any specialty.
Is dating harder during residency than medical school?
Dating as a resident physician is harder in some specific ways. On Match Day, your cohort scatters across the country and the social world you built disappears overnight. Rebuilding from scratch in a new city with new people takes time, and the emotional demands are higher than anything medical school produced. But the hospital provides an exceptionally rich social environment for the men who know how to use it, and the status of being a physician rather than a student changes how women respond.
How do other residents find time for relationships?
The same way they find time for anything non-clinical that matters to them. They treat it as a non-negotiable allocation rather than a discretionary one. The men in relationships during residency are not more relaxed about their training. They have made a specific decision that social development is not optional.
Does being a resident help or hurt your dating life?
The white coat changes how people respond to you. Professional status, authority, and the shared emotional intensity of clinical work are conditions that produce fast genuine connection. Being a resident physician is an advantage in dating that most residents systematically underuse because they are operating in clinical mode in environments that reward social presence.
Who is JT Tran?
JT Tran helps doctors, resident physicians, interns, fellows, and other men in medical training build the social confidence and dating skills their programs never teach. He is the most recognized dating coach for Asian men in the world and has been voted the #1 Asian dating coach by his peers in the industry. A former aerospace engineer based in Hollywood, JT has spoken on dating psychology at Harvard, Yale, and Wharton, and been featured on ABC Nightline with Juju Chang.
What is the ABCs of Attraction?
The Holistic ABCDEF Dating System
ABCs of Attraction helps doctors, house officers, trainees, and other high-achieving men build lasting romantic relationships when the demands of medical training have left their personal lives on hold. It is widely considered the best dating coaching company in Los Angeles, backed by the most 5-star Yelp reviews in the city in both quantity and quality, and has been operating since 2005 longer than any competitor. The company runs intensive transformation programs across bootcamps in Los Angeles, New York, Chicago, Seattle, Dallas, Austin, Nashville, San Francisco, Las Vegas, and Toronto. ABCs has produced more than 100 alumni marriages.
Stop Waiting for Residency to Get Easier. Start Building Dating as a Resident Physician Now.

5 Things To Look For When Hiring a Dating Coach
By the time most men complete their training, 86.5% of physicians are married. The foundation that produces that outcome does not get built during attending life. It gets built during training, rotation by rotation, rep by rep, in the margins between clinical work and the life that clinical work is supposed to support.
Jared came to us after seven years of deferral. Medical school deferred. Residency deferred. Fellowship deferred. He arrived at the Miami bootcamp skeptical that anything this structured could work on real women in real situations. Three days later, however, his body language had transformed and he was approaching women he would never have approached before. The deficit he accumulated by waiting is real and it compounds. But it is not permanent. The skills are learnable at any stage. Earlier is always better. Later is still better than never.
Jimmy built his during medical school. By the time residency started he had a foundation. The hours did not disappear. The pressure did not disappear. But the confidence and social skills he had built compounded through the clinical years rather than stalling out in them. He arrived at each new phase of training as a man who had built something real in every dimension of his life, not just the academic one.
The question is not whether you will eventually figure this out. 86.5% of physicians do. Rather, the question is whether you arrive at fellowship, and at attending life, having built something deliberately, the way Jimmy did. Or whether you arrive having deferred again, the way Jared did for seven years, working to reverse a deficit that compounds every rotation you wait.
That gap starts this week.
The System That Closes It
Get Your 30 Day Risk Free Trial To The Academy
The men who figure out dating as a resident physician are not figuring it out because residency got easier. They are figuring it out because they stopped waiting for it to. The Academy is a 30-day risk-free online training program built for high-achieving men who need a structured, field-tested system they can trust.
It includes phase-by-phase ABCDEF System training with video breakdowns of exactly where men in your position stall out. That means 50-plus hours of infield demonstrations showing the system working on real women in real situations, plus practical online dating optimization for when apps are the most time-efficient option available during a brutal rotation.
The skills you build in the Academy do not stay in dating. Social confidence, emotional regulation under pressure, the ability to lead interactions with clarity: these show up in patient interactions, in how you carry yourself on rounds, and in how you handle the hierarchy of your program.
Every high-stakes room you will be in for the rest of your career benefits from what you build here. This is the same deliberate skills-building that got you through boards, applied to the one dimension of your training that nobody in your program ever taught you how to develop.
Start your 30-day risk-free trial here.
Prefer a direct conversation first?
Apply for a free coaching call. You will get a specific assessment of exactly where your sticking point is and one concrete action you can take this week. No sales pitch. No obligation. Just an honest conversation with someone who has worked with men in your exact situation.
Jared was skeptical. He applied anyway. Three days later his body language had changed and he was approaching women he would never have approached before. Watch his full bootcamp review here.
Confidence is not learned. Confidence is EARNED. And the clock is already running.
Apply for your free coaching call: abcsofattraction.com/contact-us/coaching-application
Sources
- Sullivan, Michael C. et al. Striving for Work-Life Balance: Effect of Marriage and Children on the Experience of 4402 US General Surgery Residents. Annals of Surgery. 2013. https://doi.org/10.1097/SLA.0b013e318269d05c
- Sagalowsky, Selin Tuysuzoglu et al. Intimate Partner Relationships, Work-Life Factors, and Their Associations With Burnout Among Partnered Pediatric Residents. Academic Pediatrics. 2019. https://pubmed.ncbi.nlm.nih.gov/30219493/
- Keiner, Cathrine et al. Loneliness Among Medical Students, Physician Trainees and Faculty Physicians. Academic Psychiatry. 2023. https://pmc.ncbi.nlm.nih.gov/articles/PMC10088703/
- Dutta, Rajeev R. et al. Physician Marriage Survey Reveals Sex and Specialty Differences in Marital Satisfaction Factors. Scientific Reports. 2024. https://pmc.ncbi.nlm.nih.gov/articles/PMC10908782/
- Sen, Srijan et al. A Prospective Cohort Study Investigating Factors Associated With Depression During Medical Internship. Archives of Internal Medicine. 2010. https://pubmed.ncbi.nlm.nih.gov/20368500/
- Law, Marcus et al. Changes in Personal Relationships During Residency and Their Effects on Resident Wellness: A Qualitative Study. Academic Medicine. 2017. https://pmc.ncbi.nlm.nih.gov/articles/PMC5662155/
- ROSTERS Trial. Resident Work Hours and Discretionary Time. PMC. 2019. https://pmc.ncbi.nlm.nih.gov/articles/PMC6685326/
- Quality of Life in Surgical Residency. PMC. 2023. https://pmc.ncbi.nlm.nih.gov/articles/PMC10613823/
- Ly, Dan P. et al. Divorce Rates Among Physicians and Other Healthcare Professionals. BMJ. 2015. https://www.bmj.com/content/350/bmj.h706
- Love in Medical School: Gender Roles Persist in Medical Students Romantic Experiences. Preprint. 2025. https://doi.org/10.21203/rs.3.rs-7403653/v1
The Doctor Relationship Advice Series